Healthcare has tremendous power to do good, but its very complexity can also bring complications. Nowhere is that clearer than when patients are moving from one care setting to another.
A September 2008 report in the American Journal of Nursing captured the problem well. As patients move between settings, care gaps can appear because of “poor communication, incomplete transfer of information, inadequate education of older adults and their family caregivers, limited access to essential services, and the absence of a single point person to ensure continuity of care…”
Those gaps can be particularly problematic for patients with multiple chronic medical conditions who are heading to long-term care facilities (LTCs). A 2016 study in Pharmacy & Therapeutics cited studies showing that “information on discharge summaries and transfer/referral forms does not match for more than 50% of LTC admissions, with at least one medication discrepancy in 70% of all admissions.”
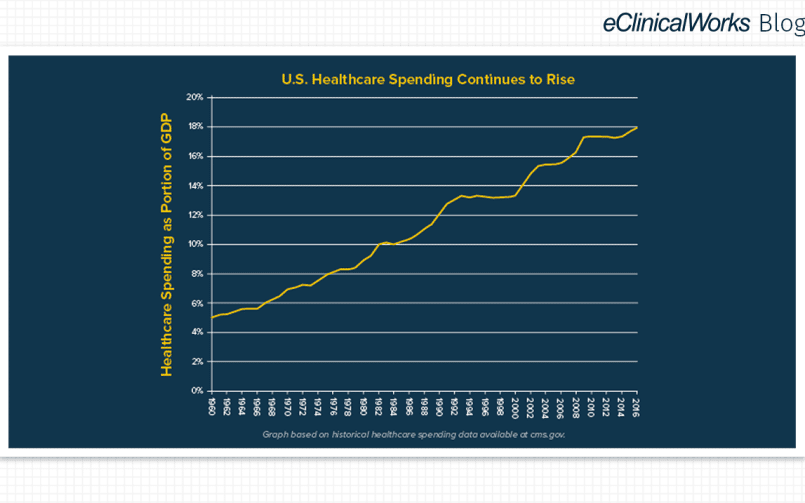
The consequences of these gaps are captured in a general way by hospital readmission rates, which drive up the cost of care and take a toll on patient health.
For MMR Healthcare of Boynton Beach, Florida, achieving a lower hospital readmission rate has been a priority. The practice has met their goal thanks in part to the use of the Transition Care Management (TCM) module from eClinicalWorks. Check out MMR Healthcare’s Success Story.
“There are some serious conditions that keep repeating themselves just because we don’t utilize the data that is available to us to change those outcomes.”
– Dr. Martha M. Rodriguez, founder, MMR Healthcare
With a large number of geriatric patients, Dr. Rodriguez recognized that having a tool for better tracking of patients between settings would be useful. What she didn’t expect was getting a more accurate idea of the reasons for hospital readmissions.
“To our surprise,” she said, “we found out that CHF (chronic heart failure), falls, and flu were our biggest problems. Using that data, we created a CHF clinic in our office.”
The result? Readmissions due to CHF fell to zero. Patients with CHF were provided with more education about diet and health, what to avoid when dining out, and were supplied with emergency medication kits to prevent trips to the emergency room. Working with a local college’s pharmacy school, MMR Healthcare educates patients about medication adherence and the proper administration of insulin. And the practice’s overall readmission rate dropped to 10-12%, well below the national average.
As this chart from HHS’s Agency for Healthcare Research and Quality shows, readmission rates vary depending upon a patient’s procedure, diagnosis, and payer. But MMR Healthcare’s overall performance exceeds readmission rates across the spectrum.
“We could never have done that had we not identified the patients that needed to be followed from hospital day one to the 30 days following discharge with a system for the collection and management of the data.”
– Dr. Martha M. Rodriguez, founder, MMR Healthcare